

Background. Myeloma patients reaped immense benefit from the introduction of new classes of drugs over the last decades. This improvement, however, was much less marked in patients with translocation 11;14 [t(11;14)], a group in which immunomodulatory drugs (IMiDs) and proteasome inhibitors (PIs) - the two most important pillars of current myeloma care - are less effective. This subgroup of patients used to be known for their relatively slow pace of progression often experiencing long plateau phases following autologous stem cell transplantation (ASCT), whereas at the same time t(11;14) is also disproportionately prevalent in difficult to treat clinical entities such as plasma cell leukemia or AL amyloidosis. Venetoclax, a selective bcl-2 inhibitor first approved for CLL was investigated for the treatment of relapsed myeloma patients and although it failed to show benefit for myeloma patients as a whole, t(11;14) patients showed exceptional responses, thus paving the way towards the first genetically targeted treatment in myeloma. As a result, its off label use is on the rise, even though clinicians have to face unanswered questions regarding the right dosage and therapy length, as well as the potential for adverse events (AEs), especially infections. Real world data could help elucidate its optimal use, but is as of yet very limited.
Aims and methods. We addressed all Hungarian centers treating myeloma to evaluate the efficacy and safety of venetoclax, collecting data about the treatment duration, AEs, dose modifications and treatment discontinuations, and analysed response rates as well as progression free survival (PFS).
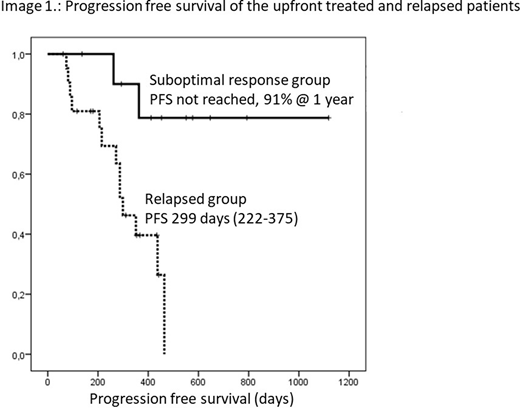
Results. 33 patients were reported from 7 Hungarian sites. After the initial analyses, we identified two distinct rationales for venetoclax treatment. 22 patients were relapsed and heavily pretreated with an average of 4.5 prior lines; here venetoclax was chosen as ultimum refugium. In this group, combination partners were bortezomib-dexamethasone (VelDex) in 14 patients, 5 had dexamethasone only, one VRd, one DRd and one Kd. Considering the highly pretreated nature of this group, the overall response rate was a remarkably high 95% with 40.9% partial, 31.8% very good partial, and 22.7% complete responses. Treatment mostly continued until progression. The median PFS and OS calculated from venetoclax initiation were 299 and 437 days. The most common AEs were cytopenias and infections reported in 8 and 6 patients with 1 fatal infection.
In the second group, 11 patients received venetoclax after a suboptimal initial response (6 PR, 4 SD, 1 PD) to their first line IMiD+PI combination with the goal of further tumor elimination preceding ASCT. Remarkably, although the length of venetoclax treatment was short - median 2 cycles -, all 11 patients deepened their response to at least VGPR and 7 to CR. 9 patients had ASCT converting 2 further VGPRs into CR, so at the end of the planned protocol 10 of the 11 patients had CR. Venetoclax was combined with VelDex in 9 and VTD in 2 cases, the one year PFS and OS were 91 and 100%, with no venetoclax related AEs reported.
An important aspect of our analysis was the question of venetoclax dosing, as the appropriate dose in this indication is not yet clear. Reflecting this uncertainty, as well as funding difficulties with this off-label drug, only one patient received 800 mg dose as seen in the Bellini trial; one received 600 mg daily, with all others taking 400 mg or less. To counteract this lower daily dose available, some centers employed a combination with clarithromycin, a strong CYP3A inhibitor known to increase venetoclax serum levels two- to threefold. Where available, serum venetoclax levels were monitored to ensure serum levels comparable to regular dosing.
Another point to emphasize is that 5 patients in the relapsed, and another 2 in the frontline group had deletion 17p, usually resulting in refractoriness to standard treatments. Among these patients however, 5 reached VGPR, 1 PR, and only one progressed on venetoclax treatment. Some responses proved lasting especially in the frontline group.
Conclusion. Our results highlight the importance of targeted treatments in multiple myeloma. We experienced lasting responses in quadruple-refractory patients. In the newly diagnosed group where the depth of pre-ASCT response has a big impact on PFS, venetoclax may have a role converting suboptimal responses into CRs by eliminating residual disease.
Illés:Takeda, Seattle Genetics: Research Funding; Novartis, Janssen, Pfizer, Roche;: Other: Travel, Accommodations, Expenses; Celgene, Janssen, Novartis,Roche, Takeda: Consultancy; Janssen, Celgene, Takeda, Novartis Pharma SAS, Pfizer Pharmaceuticals Israel, Roche;: Consultancy, Honoraria.
venetoclax use in t(11;14) myeloma which is not yet licensed

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal